Cochrane Database Syst Rev. 2013 Mar 28;3:CD004310. doi: 10.1002/14651858.CD004310.pub3.
% x: i! ^1 p2 W# B+ x$ ~& C W* kMegestrol acetate for treatment of anorexia-cachexia syndrome." N% G6 G4 S* d' Y; i
Ruiz Garcia V1, López-Briz E, Carbonell Sanchis R, Gonzalvez Perales JL, Bort-Marti S.$ X0 g5 s6 y! \- w8 z' ?& X
Author information
# w% K" g9 d. `2 qAbstract
' Z2 O5 N7 V2 c2 c3 XBACKGROUND:4 h5 L5 k: Z( |
This is an updated version of a previously published review in The Cochrane Library (2005, Issue 2) on 'Megestrol acetate for the treatment of anorexia-cachexia syndrome'. Megestrol acetate (MA) is currently used to improve appetite and to increase weight in cancer-associated anorexia. In 1993, MA was approved by the US Food and Drug Administration for the treatment of anorexia, cachexia or unexplained weight loss in patients with AIDS. The mechanism by which MA increases appetite is unknown and its effectiveness for anorexia and cachexia in neoplastic and AIDS (acquired immunodeficiency syndrome) patients is under investigation.
' h: u- b% }- N6 w# \9 ?1 D+ YOBJECTIVES:4 v0 c* M% ]9 `9 g2 q, _: ^
To evaluate the efficacy, effectiveness and safety of MA in palliating anorexia-cachexia syndrome in patients with cancer, AIDS and other underlying pathologies.
9 h7 p+ y- ]) ^: s6 sSEARCH METHODS:7 O& F; O% `5 y, c4 R
We sought studies through an extensive search of electronic databases, journals, reference lists, contact with investigators and other search strategies outlined in the methods. The most recent search for this update was carried out in May 2012.
6 b7 D& @4 `6 R s6 m& hSELECTION CRITERIA:
: e+ }; ?/ e$ t6 G' n' i% z( }5 S; IStudies were included in the review if they assessed MA compared to placebo or other drug treatments in randomised controlled trials of patients with a clinical diagnosis of anorexia-cachexia syndrome related to cancer, AIDS or any other underlying pathology.
& B' U: e, M' l2 {5 uDATA COLLECTION AND ANALYSIS:. u" p. ~6 @: D' ~* Y! r
Two independent review authors conducted data extraction and evaluated methodological quality. We performed quantitative analyses using appetite and quality of life as a dichotomous variable, and analysed weight gain as continuous and dichotomous variables.
% \4 {+ P4 P3 ?7 gMAIN RESULTS:
% ?/ A4 b! D3 } F8 D2 l6 \We included 35 trials in this update, the same number but not the same trials as in the previous version of the review. The trials comprised 3963 patients for effectiveness and 3180 for safety. Sixteen trials compared MA at different doses with placebo, seven trials compared different doses of MA with other drug treatments and 10 trials compared different doses of MA. Meta-analysis showed a benefit of MA compared with placebo, particularly with regard to appetite improvement and weight gain in cancer, AIDS and other underlying conditions, and lack of benefit in the same patients when MA was compared to other drugs. There was insufficient information to define the optimal dose of MA, but higher doses were more related to weight improvement than lower doses. Quality of life improvement in patients was seen only when comparing MA versus placebo but not other drugs in both subcategories: cancer and AIDS. Oedema, thromboembolic phenomena and deaths were more frequent in the patients treated with MA. More than 40 side effects were studied., i2 x r0 { U! d% W B3 U7 d
AUTHORS' CONCLUSIONS:
1 q( [- P' P$ w! n, l: ZThis review shows that MA improves appetite and is associated with slight weight gain in cancer, AIDS and in patients with other underlying pathology. Despite the fact that these patients are receiving palliative care they should be informed of the risks involved in taking MA.+ ^. V8 b8 z, J$ D3 y
|
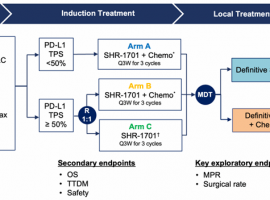 25%肺癌患者变不可手术为可手术,新
作者:seacat
驱动基因阴性的III期非小细胞肺癌的治疗颇具挑战,能否手术切除没有一致
25%肺癌患者变不可手术为可手术,新
作者:seacat
驱动基因阴性的III期非小细胞肺癌的治疗颇具挑战,能否手术切除没有一致
 聚焦2025 ASCO 前列腺癌新进展,从循
作者:Tony男人一旦上了年纪,总有些难以启齿的尴尬,如尿频、尿急、尿不尽……很多人
聚焦2025 ASCO 前列腺癌新进展,从循
作者:Tony男人一旦上了年纪,总有些难以启齿的尴尬,如尿频、尿急、尿不尽……很多人
 20前插+Pik3ca,请教各位战友、老师
肺腺癌iVb期,首次基因检测发现是20前插+Pik3ca,ki-67 10%~20%。
刚刚进行了一次培美
20前插+Pik3ca,请教各位战友、老师
肺腺癌iVb期,首次基因检测发现是20前插+Pik3ca,ki-67 10%~20%。
刚刚进行了一次培美
 需要加论坛患者群的朋友们看这里
本帖最后由 青菜567 于 2024-7-22 17:38 编辑
与癌共舞小助手-29新进论坛需要进入患
需要加论坛患者群的朋友们看这里
本帖最后由 青菜567 于 2024-7-22 17:38 编辑
与癌共舞小助手-29新进论坛需要进入患
 肺癌术后五年,脑膜转移治疗三年,伏
2020年7月右上胸腔镜下肺癌根治术,术后病理(右上肺叶)周围浸润性腺癌(腺泡亚型为
肺癌术后五年,脑膜转移治疗三年,伏
2020年7月右上胸腔镜下肺癌根治术,术后病理(右上肺叶)周围浸润性腺癌(腺泡亚型为





 显身卡
显身卡


